Home
Featured
Showing item 1 of 2


Carousel Navigation
Common Conditions and Injuries




")

If this list is too long for the page, you can scroll it left and right


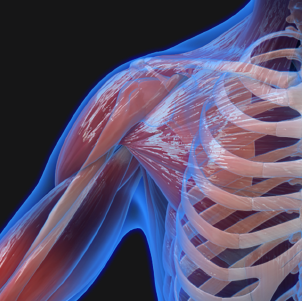
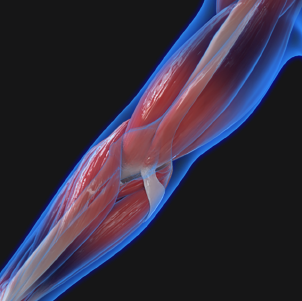
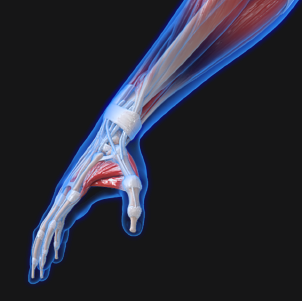
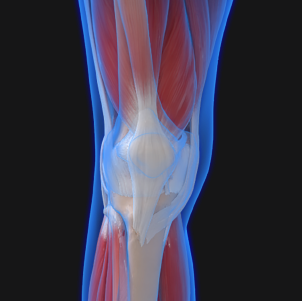
Find Information by Body Part
Select a body part to learn more about common injuries and treatment options.